
Healthcare workers tend to a patient at Providence St. Mary Medical Center in Apple Valley, California on January 11, 2021. (Photo by ARIANA DREHSLER/AFP via Gett Images)
Martin Kulldorff recently wrote the following:
For the mRNA vaccines, the big question that needs an urgent answer is whether they cause an increased risk of heart attack and/or other serious heart problems. There are many anecdotal reports, especially among young male athletes, and many VAERS reports.
He further writes:
Public health officials face a temptation to summarily dismiss anecdotal vaccine injury stories and people concerned about the publicly available VAERS reports, but in public health, we cannot do that. We must take people’s concerns seriously.
What’s an economist’s reaction to anecdotal evidence? A friend recently asked me about the statistical relevance of anecdotal evidence. My answer to him was the following. The sum of life experiences by the many leads to a picture of the whole, while a picture of the whole hides unique and varied life experiences.
No “anecdotal evidence” should be dismissed a priori, just because it has been observed over a small and/or unique sample. The questions are the same, whether about “anecdotal evidence” or “evidence over a larger sample or population”: Have we really observed a change in the pattern in our data? What kind of inferences, if any, can we make from our observations?
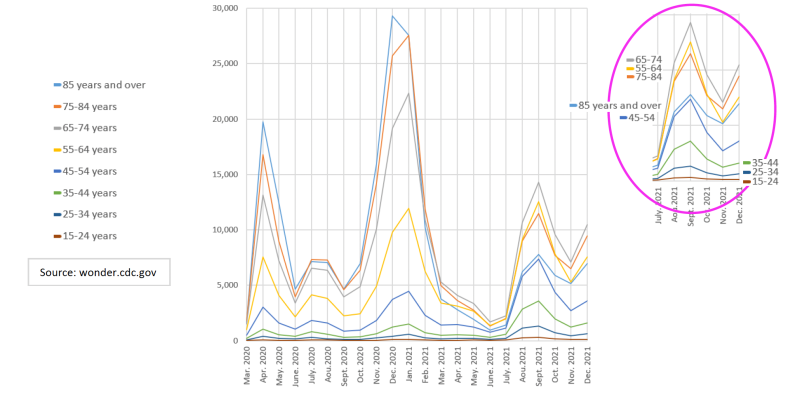
I have never paid much attention to athletes (no offense to the athletes), but I have recently paid attention to U.S. deaths. Using publicly available CDC data, I simply plotted monthly U.S. deaths, from 1999 to 2021.
To my surprise, deaths due to suicides do not show an increase in 2020-21. But we thought they did, didn’t we? Does this mean we were not paying attention to suicides before, but recent events made us more attune to the suffering of others? Or does it mean deaths of despair are found in other cause of death categories? Deaths due to accidental poisoning and exposure to noxious substances (which include accidental drug and alcohol overdose) have increased. Deaths due to homicide, and deaths due to liver diseases, have too.
Some thought April 2020 deaths were too high and justified putting our lives on hold, but January 2021 numbers were worse—the percentage death rate in 2021 is the same as it was in 2020. Why the increase in January 2021 deaths? Continued upward trend in deaths due to the increase and aging of the US population? Deaths of despair? Increased deaths due to untreated conditions in 2020? Deaths due to COVID or one of its variants? Vaccine deaths?
In 2021, death numbers have peaked at unprecedented levels, in September, for the 45-54, 35-44 and 25-34 years old. September 2021 deaths for the 65-74 and 55-64 years old were also higher than their April 2020 numbers.
Ok, so why is that significant? Let’s take the 45-54 years old group for example. Seasonal variations in deaths for this group has always been less pronounced than for the 85 years and older group, but whatever peaks they had, they still occurred mostly in January for both groups—so a 45-54 years old death peak in September is unheard of.
Why the increase in September 2021 deaths? Continued upward trend in deaths due to the increase and aging of the US population? Deaths of despair? Not consistent with a September peak of deaths. Increased deaths due to untreated conditions in 2020? Deaths due to COVID or one of its variants? Not consistent with a peak of deaths predominantly observed for “younger” age groups.
Vaccine deaths? The January 2021 peak, which is higher than the April 2020 one, is dominated by deaths from 65 years and older age groups. The September 2021 peak is dominated by 64 years and younger age groups.
But don’t those peaks also correspond to the COVID-19 ones? That’s correct.
But, while the April 2020 and January 2021 COVID-19 deaths peaks show the usual age distribution, with deaths experienced in greater numbers for older age groups, the September 2021 does not. In September 2021, recorded COVID-19 deaths show 65-74 years old died in greater numbers than 75 years and older, and COVID-19 deaths for the 45-54 years old were as high as for the 85 years and older.
This has never happened before for deaths due to respiratory diseases, from 1999 to 2019. These September 2021 peaks for “younger” age groups are consistent with the vaccine deaths hypothesis.
My motivation has always been to minimize the suffering. Even if COVID-19 had been alarming, panic certainly wouldn’t help. Even if the vaccines were harmless, denying individuals the ability to opt out, doesn’t help the ones who willingly opt for it. Am I afraid to admit COVID vaccines have caused deaths? Are you?
Republished from Brownstone Institute
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times.